
1. Initial Patient Presentation
Patient:
A 24 year old male patient with a four month history of
- Multiple seizures, two of which were described as tonic-clonic seizures. The others were focal onset seizures, characterized by loss of conciousness, rapidly followed by left hand automatisms, collapses, and return to consciousness after a few minutes
- Impaired awareness
- Severe headaches, especially after the seizures
Neurological examination showed slightly decreased attention and memory function, compared to healthy people of similar age and education. No abnormalities of motor, gait, balance, or sensory function were noted. The patient was treated with carbamazepine (200 mg, 3 x day), which did not improve the seizures. Further assessments and imaging were performed to investigate an underlying cause (see Figures 1-8).
Diagnosis:
- Left temporal pole AVM: Spetzler-Martin Grade II
- Nidus size 2.5 cm
- Multiple supply sources: mostly from the middle cerebral and posterior cerebral arteries
- Multiple drainage points including superior anastomotic vein to the superior sagittal sinus, and tributaries to the inferior petrous sinus, basal vein, and great cerebral vein
Treatment Decision:
At multidisciplinary review, the decision was made to surgically resect the AVM due to the following reasons:
- Patient had poor response to anticonvulsant treatment
- Risk of hemorrhage from this malformation remains high if not resected
- Treatment of choice for Spetzler-Martin Grade II AVMs is microsurgical resection, because this can provide immediate cure with low risk of a recurrence
The aim of the surgery is to achieve control of the seizures and to prevent a hemorrhagic episode that could lead to a neurological sequelae.
For video showing the exposure, clippings and resection of the AVM please see video at the end of the article.
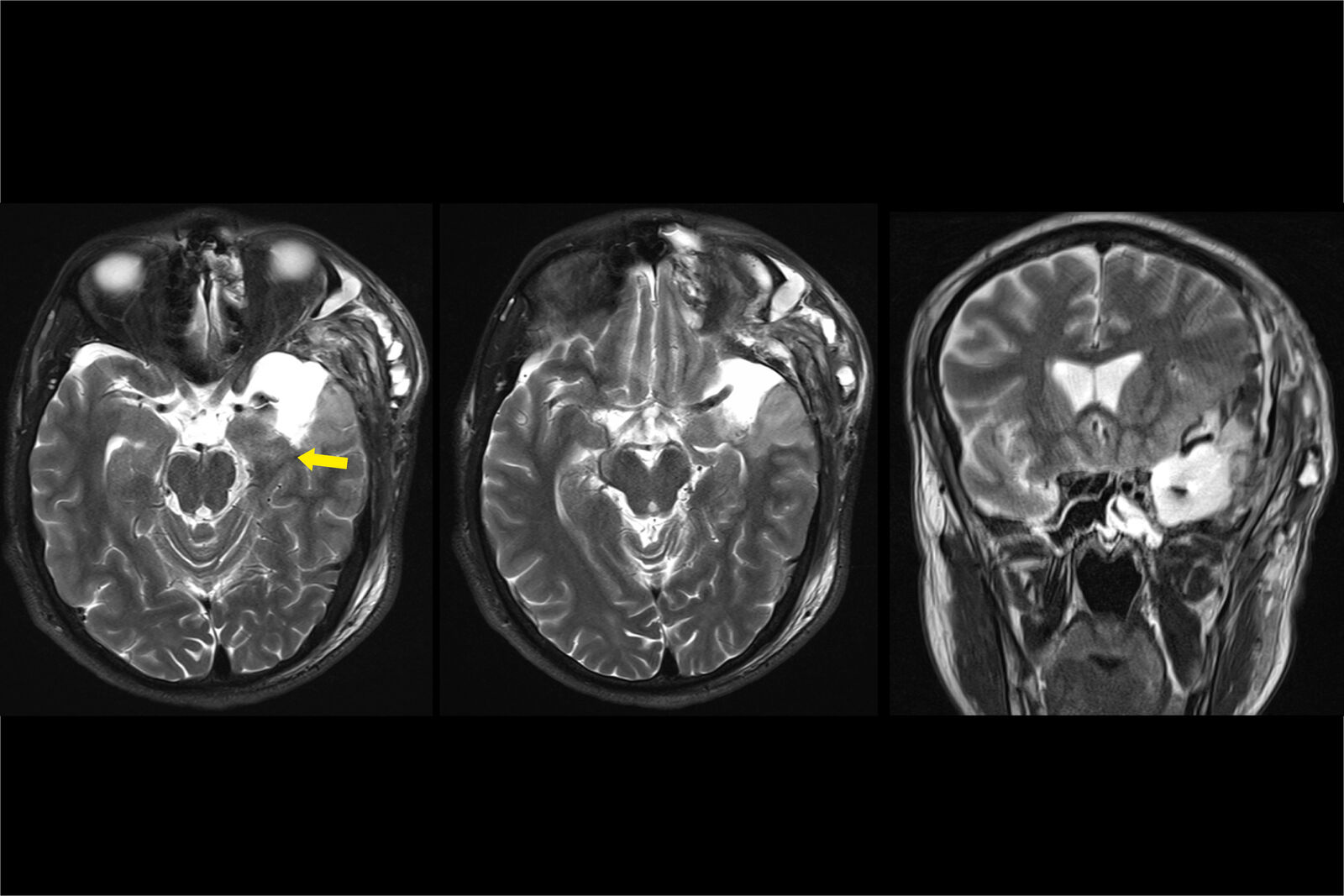
2. Pre-operative Assessment
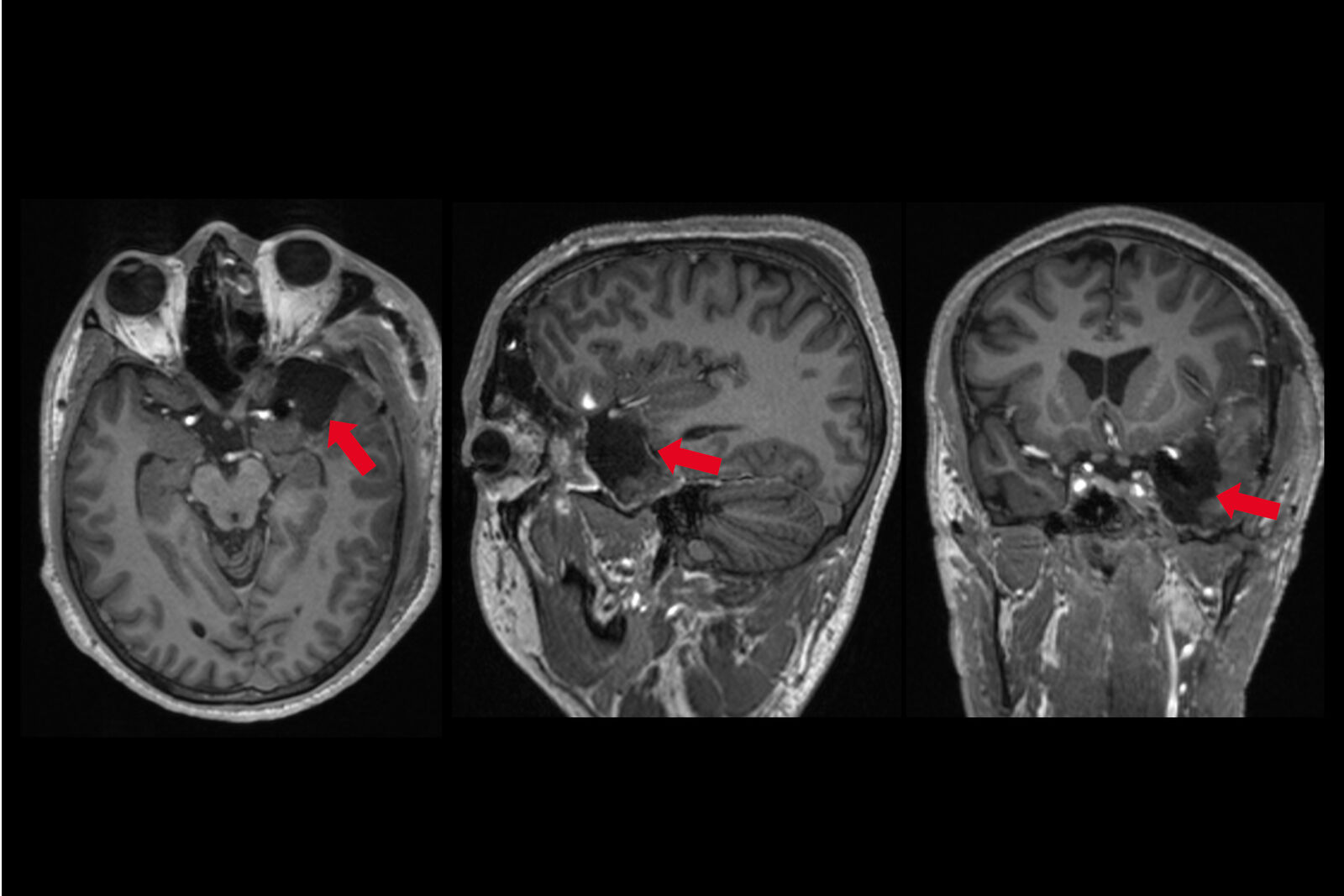
Pre-operative Imaging
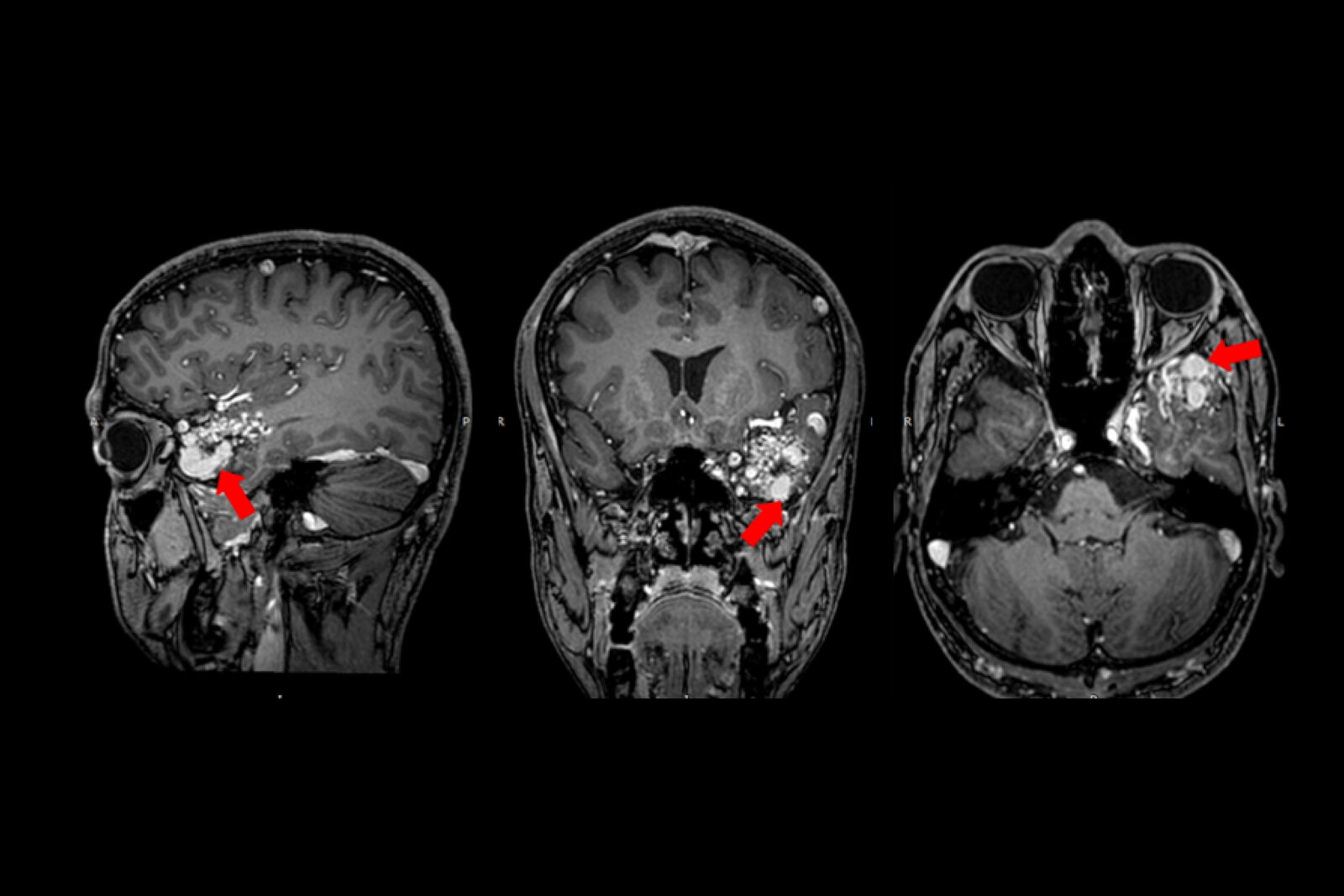

left hippocampus edema (hyperintensity signal, red arrow).
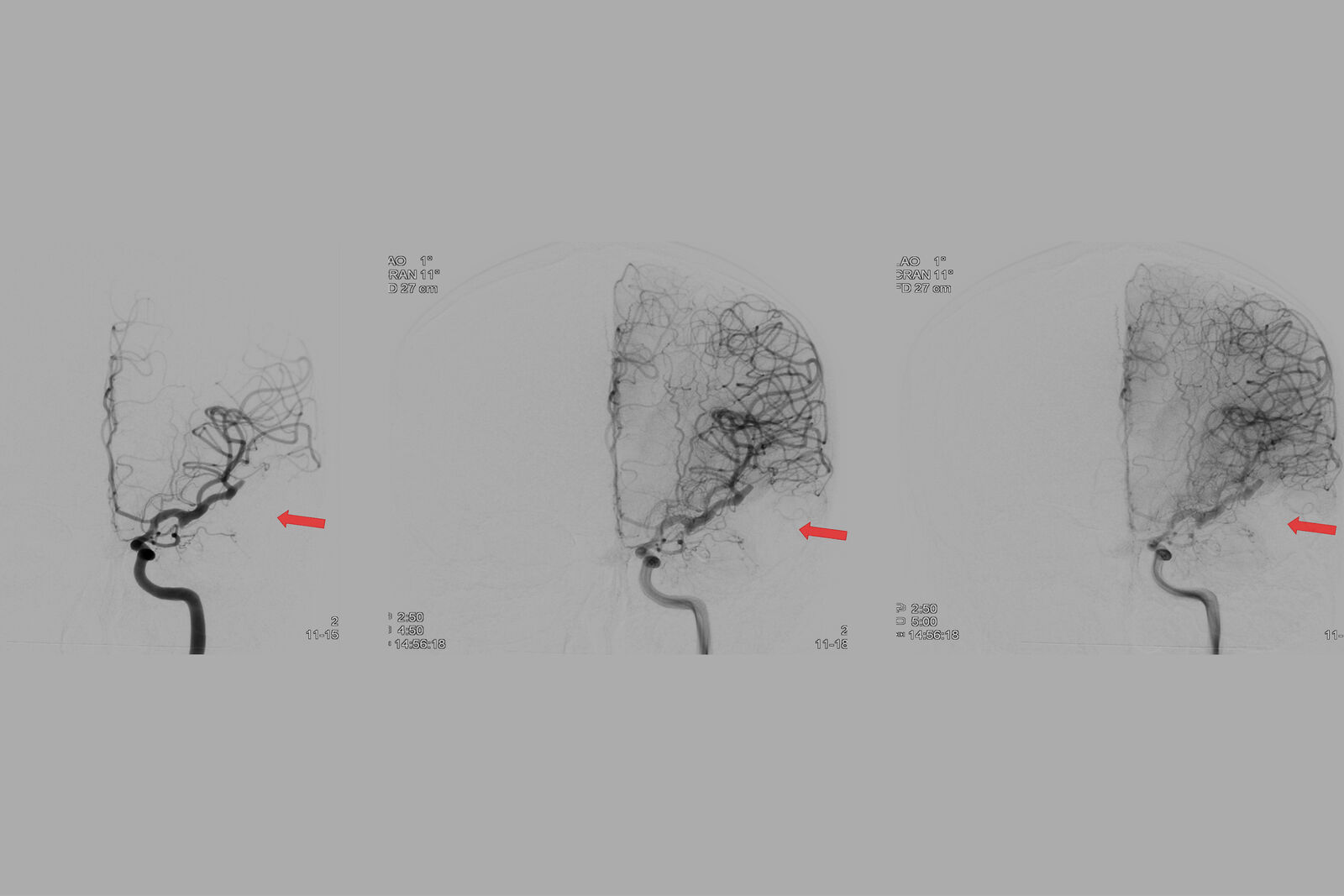
Pre-operative Imaging: AVM Supply
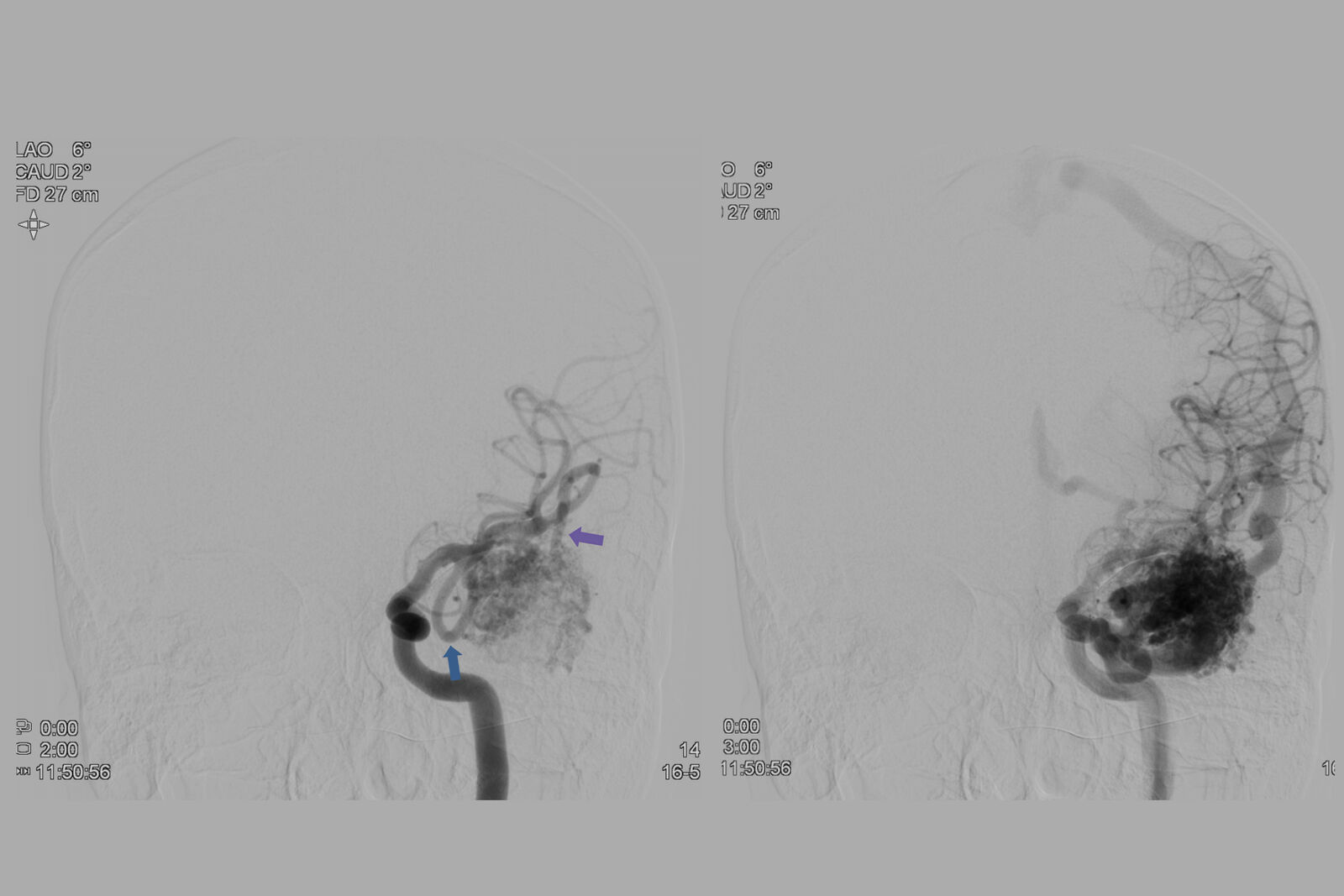
early branch (blue arrow) and terminal branches of the interior trunk (purple arrow).
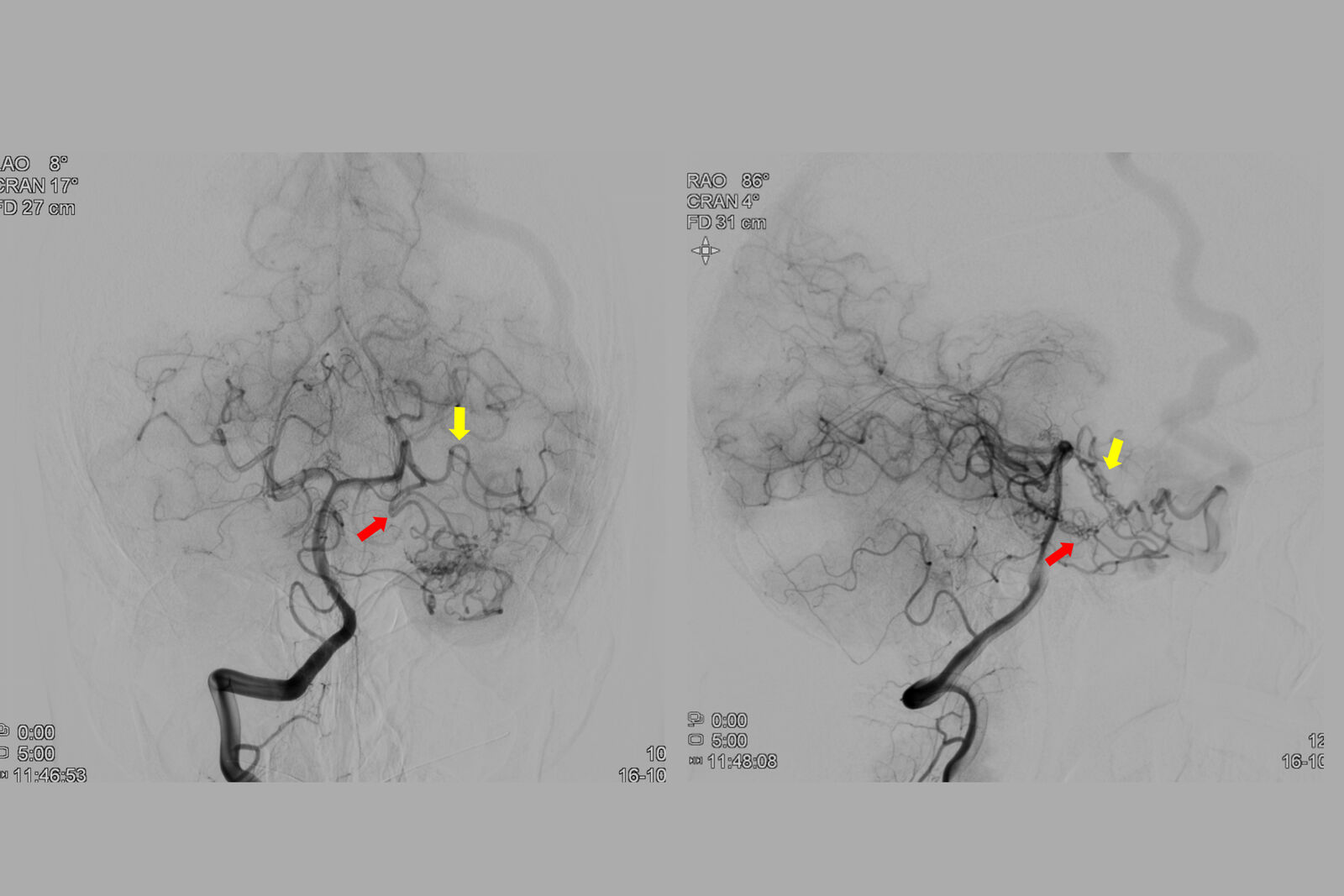
arteries (yellow and red arrows, respectively).
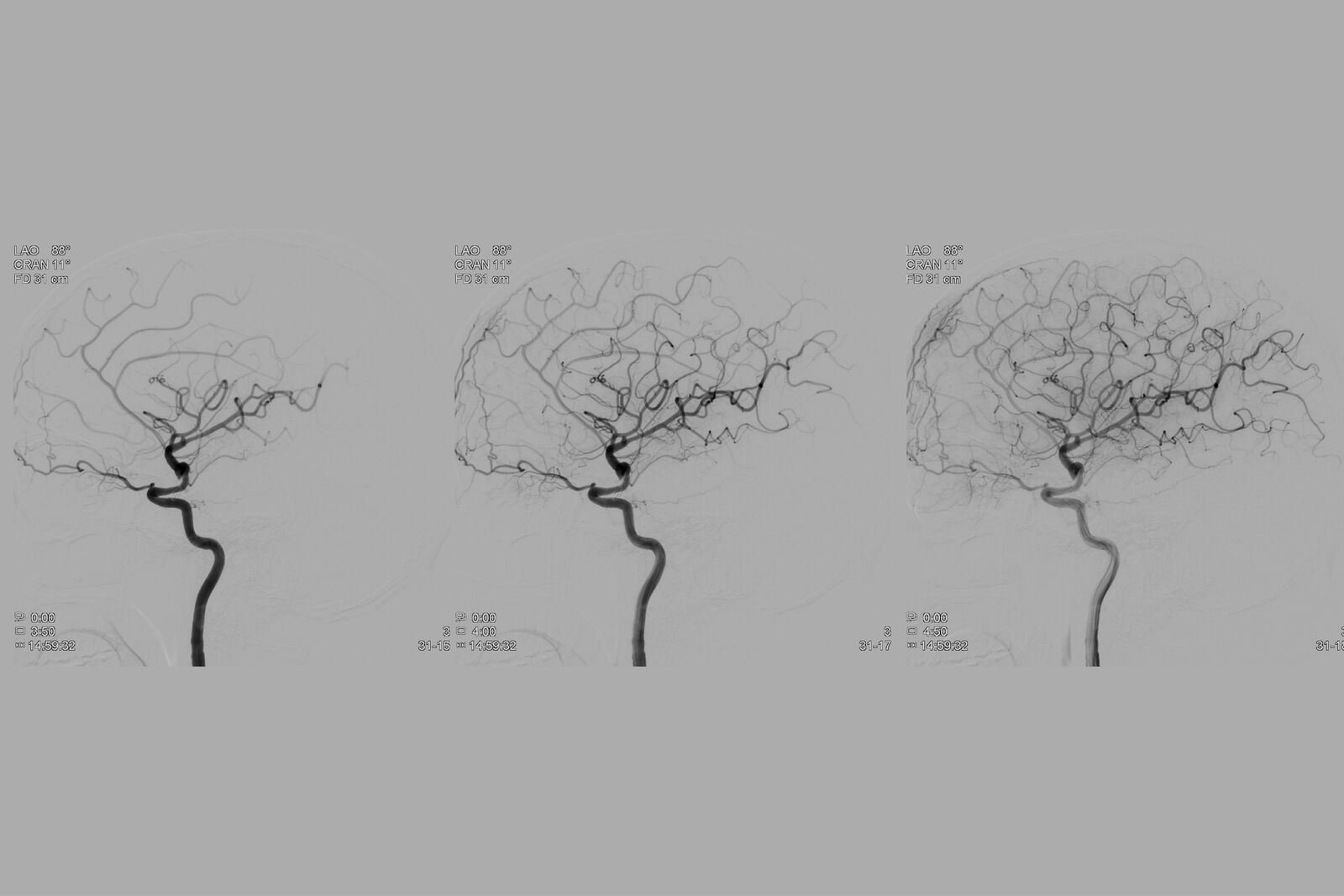
Pre-operative Images: AVM Drainage
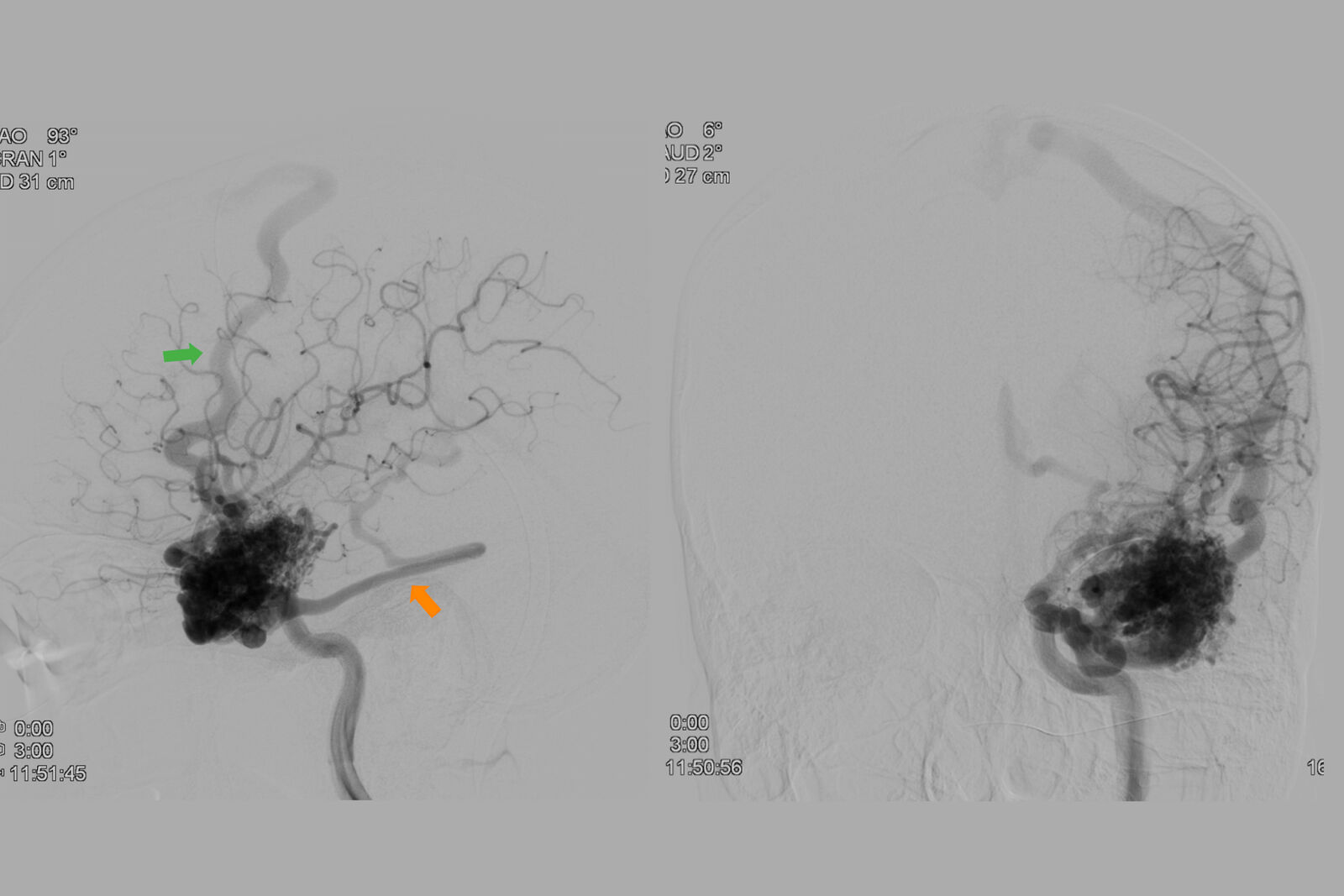
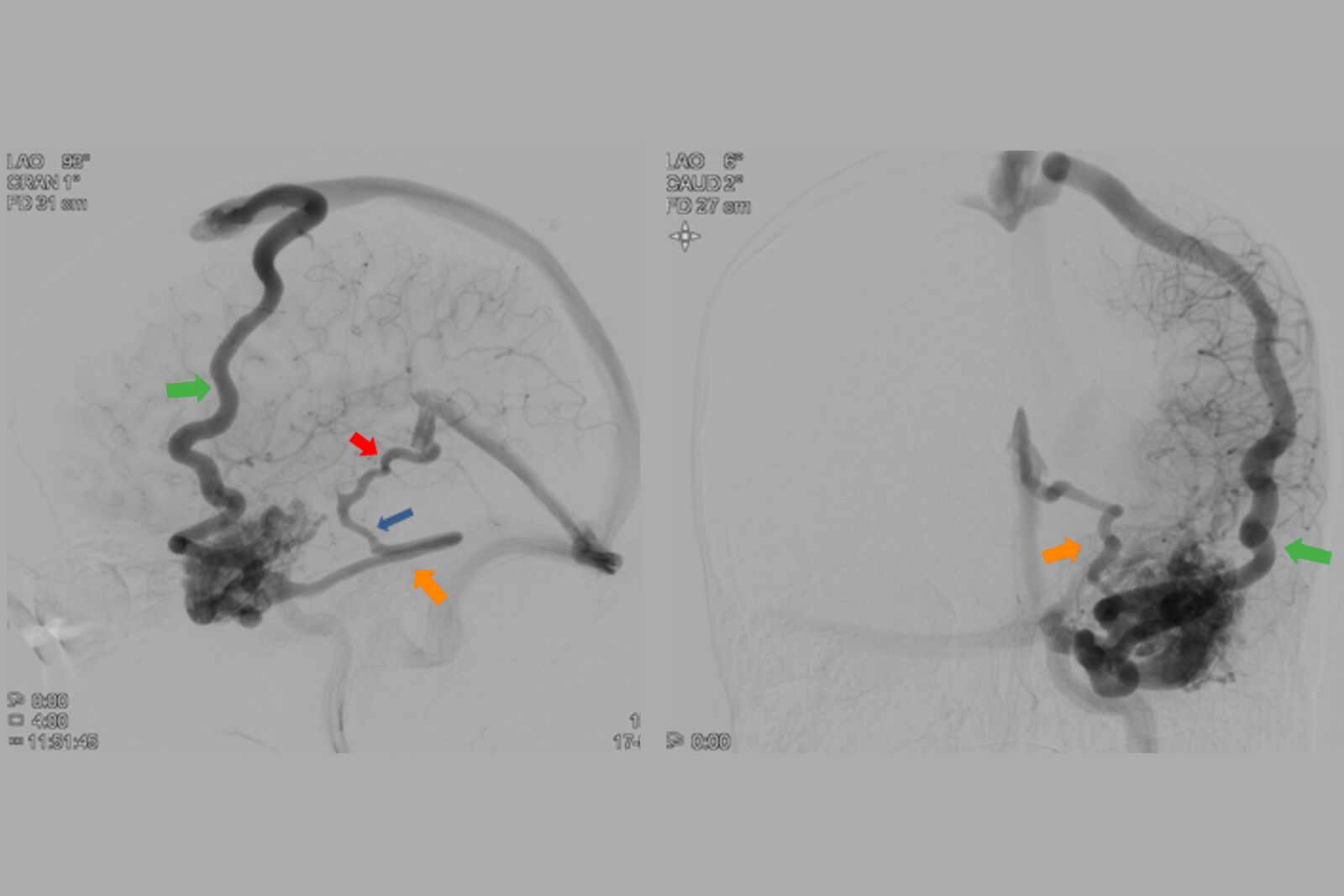
(orange arrow) were also present. The blue arrow indicates the inferior petrous sinus anastomosing with the lateral mesencephalic vein.
Pre-operative Assessment Images - Steal
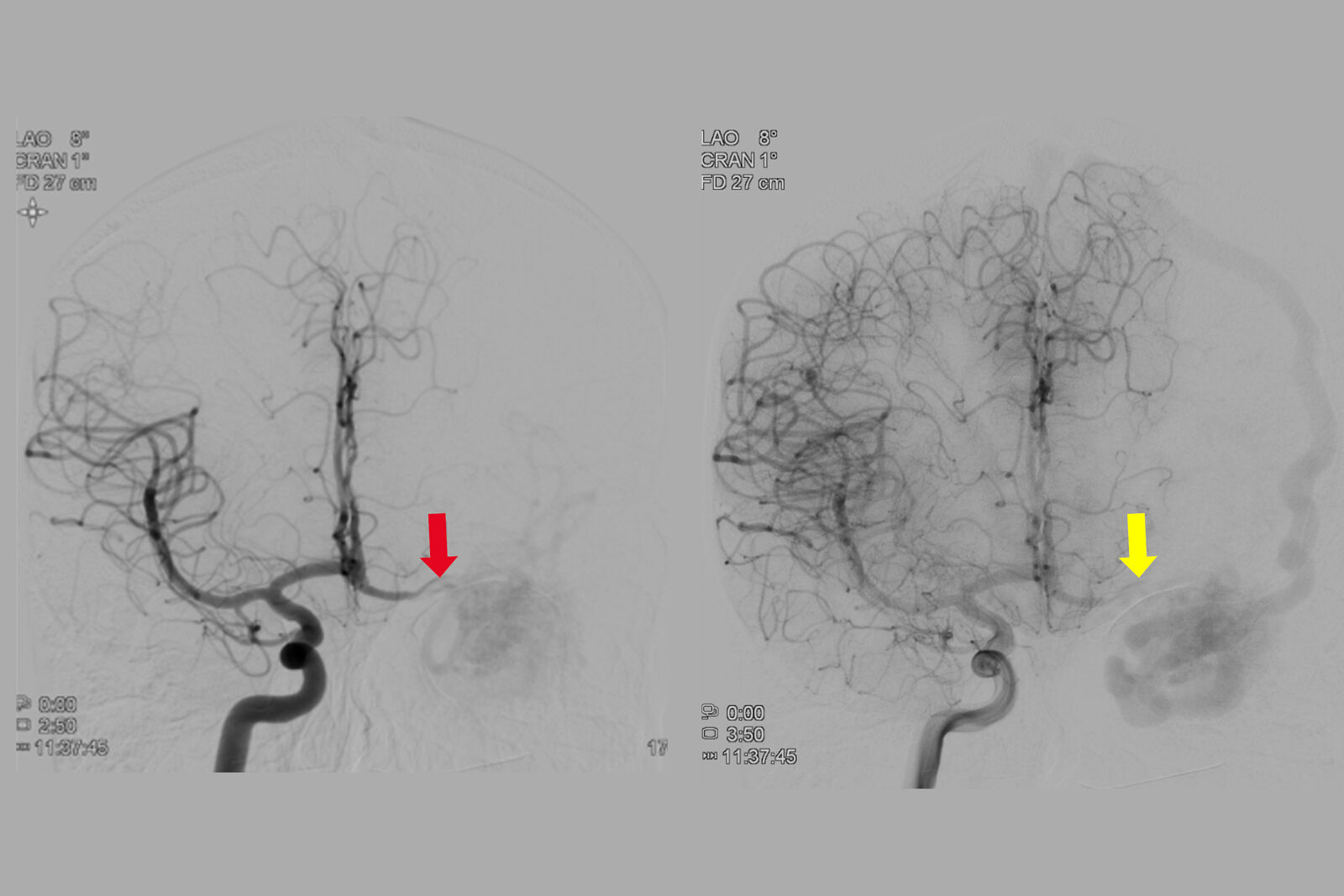
anterior cerebral artery (yellow arrow).
3. Intra-operative Course and Images
A pretemporal craniotomy was performed to take advantage of the transsylvian, lateral subfrontal, subtemporal and temporoporal corridors. With this craniotomy the superior, middle and inferior temporal gyrus, the Sylvian fissure, the inferior and part of the middle frontal gyrus were exposed.
For video showing the exposure, clippings and resection of the AVM please see video at the end of the article.
AVM First Assessment
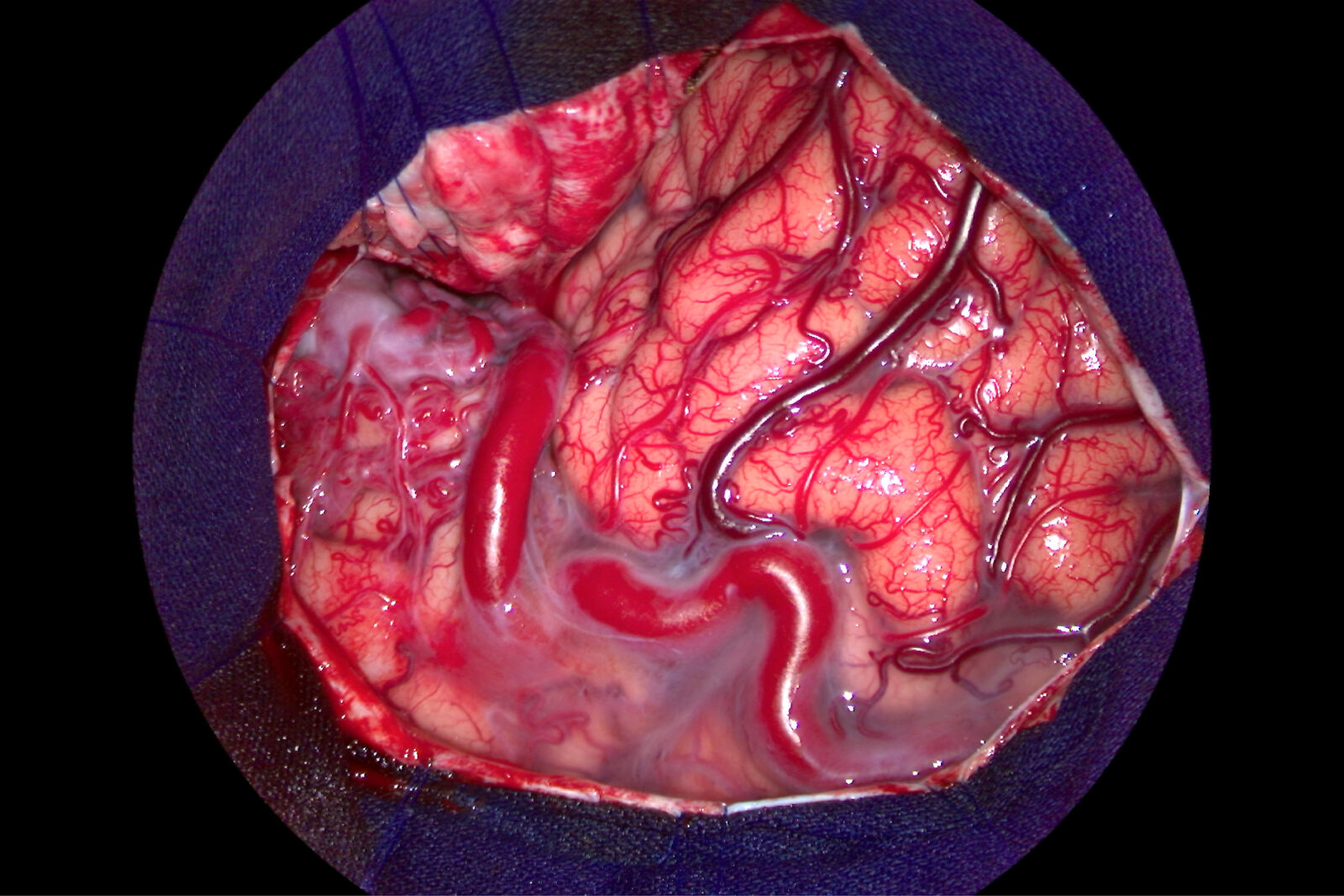
lobe and was also assessed using GLOW800.
AVM Resection
GLOW800 helped to understand the superficial configuration of the AVM and to confirm the surgical strategy that was decided earlier.
Following the initial assessment of the AVM, Prof. Chaddad opened the Sylvian fissue using sharp dissection in the arachnoid space. He separated the frontal lobe from the temporal lobe in order to gain a better exposure of the AVM and expose the middle cerebral artery, which was the principal feeder of the AVM.
GLOW800 showed the flow through the vessels and the brain parenchyma in real time, which allowed to continue working while assessing the anatomical structures.The superficial feeders and shunts were then disconnected from the AVM.
Deeper circumferential dissection was then done, coagulating and cutting off feeder vesels in order to progressively decrease the flow through the AVM.
The branches of the posterior cerebral artery were accessed through the subtemporal corridor.
GLOW800 Post AVM Exclusion
4. Post Surgery
Post Surgery Examination and Discharge:
- Patient was discharged on the eighth postoperative day with a Rankin Modified Scale of 0
- After six months, the patient has not had new seizures, and no new neurological or neuropsychological deficits.
5. Impact of GLOW800 Augmented Reality Fluorescence
One augmented view during vascular neurosurgery can improve confidence in intra-operative diagnosis
- One augmented, real-time view means no more need to recall and try to reconcile the black and white blood flow video with the natural anatomical view
- Crisp delineation helps you limit potential compromise or obstruction of surrounding perforators and small vessels
- Full depth perception and no dark peripheries supports clear spatial orientation to aid manipulation of vessels
Improved confidence in treatment
Visualization with GLOW800 AR supports each step of vascular neurosurgery procedures and also supports with post-operative imaging. For example, during AVM treatment, it helps:
- Manipulate the AVM to assess beyond the superficial anatomical view while simultaneously observing flow
- Confidently assess flow dynamics of inflow and outflow in stereoscopic view
- Assess filling and emptying of the AVM during the different phases (arterial and venous)
- View changes in filling rate and time of the AVM as feeders and fistulas are disconnected and as surgery progresses
- Confirm complete exclusion and/or excision of the AVM from normal circulation and evaluate the patency of vessels.
A fundamental tool for the future practice and training in neurosurgery
In the binocular image injection (CaptiView) better defining (lowering) the dose of Indocyanine Green (ICG) was enough to generate the flow effect without saturating the view of the whole operative field. Also, the microscope’s monitor offers a perfect view, where the observer can easily understand the anatomy and the AVM exclusion strategy adopted. Image settings can be effortlessly changed, to optimize the view as needed.
Download
Download Case Study GLOW800 Augmented Reality Fluorescence in AVM Treatment (pdf)
Related Articles
-

Skull Base Neurosurgery: Epidural Lateral Approaches
Surgery of skull base tumors and diseases, such as cavernomas, epidermoid cysts, meningiomas and…
Oct 10, 2022Read article -

Digitalization in Neurosurgical Planning and Procedures
Learn about Augmented Reality, Virtual Reality and Mixed Reality in neurosurgery and how they can…
Sep 19, 2022Read article -

Augmented Reality Assisted Navigation in Neuro-Oncological Surgery
In neuro-oncological surgery, new technologies such as Augmented Reality are helping to improve…
Aug 25, 2022Read article
