
High-grade gliomas treatment & surgical management
The gold standard for high-grade glioma treatment is the usage of multi-modal therapy, consisting of surgery, chemotherapy and radiotherapy. The combination of these therapies aims to postpone tumor progression, extend patient survival and delay recurrence and patient death. The concomitant use of chemotherapy and radiotherapy can extend patient survival by 2 months compared to radiotherapy alone. Patients with complete tumor resection derive most benefit from this combination, Dr. Rezinho explains..
The role of surgery is paramount. It provides a sample of the tumor to understand its genetic markers, which are directly linked to the prognosis. The extent of resection also seems to have a direct impact on overall survival and progression-free survival.
An analysis of 500 patient series1 has shown a benefit on survival over 78.5% tumor volume resection (over 12.2 months). The most benefit on survival was observed with an extent of resection (EOR) over 98%. Another study2, looking at 1,229 patients, revealed that patients with an extent of resection of 100% survived more than patients with an extent of resection between 78 and 99% (15.2 months). When clinically feasible, it is thus advisable to favor gross total resection.
How can extent of resection be expanded intra-operatively?
Dr. Rezinho recounts how neurosurgeons have several tools at their disposal to achieve gross total resection. These include the surgical microscope and intraoperative imaging tools: intraoperative MRI, neuro-navigation and intraoperative ultrasonography.
With neuro-navigation and diffusion tensor imaging (DTI), there is a risk of brain shift which can lead to insufficient resection and neurological deficits. Intraoperative MRI can help overcome brain shift, although there can be image distortion and inaccurate target registration and other limitations. Intraoperative ultrasonography also avoids brain shift, although there are lower levels of anatomical detail and residual disease can be difficult to detect.
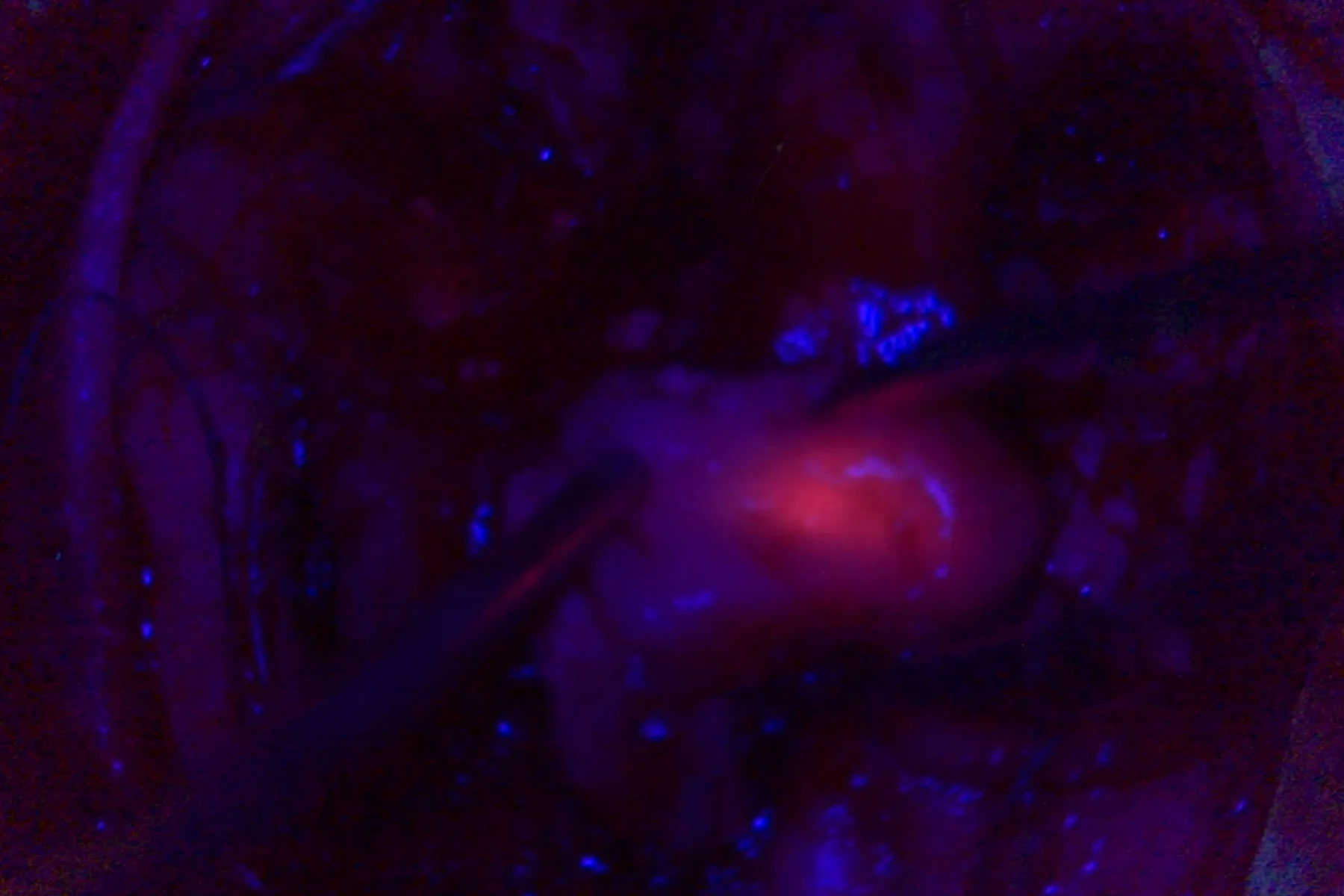
Another valuable tool is metabolic marking, with 5-ALA fluorescence. It allows the surgeon to distinguish the metabolic patterns of the tissue in order to extend the resection. 5-ALA must be administered to the patient orally 3 to 4 hours prior to surgery. The fluorescence peak occurs 6 to 8 hours after administration.

The benefits of 5-ALA fluorescence-guided surgery
A randomized controlled multicenter phase III trial3 has shown that the use of 5-ALA fluorescence-guided surgery for the resection of malignant gliomas can extend progression-free survival by 1.7 months. In addition, gross total resection was twice as probable in the 5-ALA group compared to white light (65% vs 36%), dr. Rezinho cites during her webinar.
However, there was great variability from one center to another and more experienced centers were able to achieve 90% gross total resection. 5-ALA is a supporting tool: efficacy in attaining gross total resection depends on the surgeon’s training, experience and proximity of the glioma to the eloquent cortex.
5-ALA also has a certain number of limitations, including photobleaching effects, blind spots and glioblastomas tumor heterogeneity with necrosis and hemorrhage. It is also important to be cautious with patients with neurological deficits, to avoid aggravation.
The importance of planning to avoid Iatrogenic neurological deficit
Knowledge of tumor location and surrounding brain is essential to avoid neurological deficits when performing glioma resection. The advances in imaging allow for the identification of not only the cortical location of the tumor dr. Rezinho says, but also the relation to white matter tracts and the degree of invasiveness. Intraoperative stimulation mapping is also an important tool to define the best approach, reduce severe neurological deficits and expand gross total resection. This can be done in collaboration with a neuropsychologist, who helps monitor language and other cognitive skills in the operating room.
Surgical approach to extend high-grade glioma resection
The first step is to evaluate tumor resectability. An MRI confirms the anatomic location, while diffusion tensor imaging (DTI) shows whether tracts are destroyed, infiltrated or displaced. It is also helpful to try to evaluate the response to steroids. There are tumors for which gross total resection cannot be achieved, and as such must not be attempted.

If the conclusion of the evaluation is that gross total resection is not possible, cytoreduction surgery can be considered with a focus on neurological preservation and the use of intraoperative imaging. If the tumor is not around the eloquent brain and the evaluation concludes that gross total resection is attainable, cytoreduction can be performed leveraging 5-ALA and intraoperative imaging. If the tumor is near the eloquent brain and gross total resection is possibly attainable, cytoreduction and neurological preservation should be balanced.
When planning resection around the eloquent brain, it is key to understand which tracts are involved. A useful tool is Dr. Michael Lawton’s AVM “box technique” with the identification of walls. During the planning phase, it is also critical to choose mapping paradigms and plan with the neuropsychologist and neurophysiologist, deciding if the patient will be awake or asleep.
For the surgical resection, it is important to start with anatomical landmarking, using navigation and cortical mapping. Injecting the navigation in the microscope can help identify the tumor margins.
During superficial resection, vessels must be considered in order to preserve them as much as possible. It is also important to perform debulking until the sulci deep end. When going to the depth of the tumor, a helpful approach is to alternate 5-ALA resection on the tumor margin with white matter mapping wall by wall.
After resection, Dr. Rezinho concludes, it is good practice to confirm gross total resection and check for tumor residue, for example with ultrasonography. An early post-operative MRI also helps evaluate surgery results and determine if a second-look surgery is required.
Want to learn more? Watch the full webinar presented by Dr. Carla Reizinho and see the clinical cases she shared.
Note: Please note that off-label uses of products may be discussed. Please check with regulatory affairs for cleared indications for use in your region. The statements of the healthcare professionals included in this symposium reflect only their opinion and personal experience and not those of Leica Microsystems. They also do not necessarily reflect the opinion of any institution with whom they are affiliated
 case.")


