1. Introduction
Since the development of optical coherence tomography (OCT) in the 1990s [1], this technology has undergone several increments that have improved scanning speed and image quality [2-5]. One of the most significant improvements in this technology was its entry into the operating room [6-8].
There are currently three commercially available intraoperative OCT brands. Leica is one of the suppliers offering three different OCT models. The EnFocus Ultra-HD OCT and the EnFocus Ultra-Deep OCT were both launched in 2016. The EnFocus intraoperative OCT, built into the Proveo 8 ophthalmic microscope, was launched in 2020.Intraoperative OCT essentially has two indications: retinal surgery and corneal surgery. The place of intraoperative OCT in these two indications is established and no longer needs to be proven [6-10].
I have been using the Proveo 8 microscope for two years and intraoperative OCT for a year. I initially acquired this device for retinal surgery but quickly realized that it could be greatly beneficial in an indication that is quite common: cataract surgery. Here, I will share my experience with intraoperative OCT in this everyday surgery and explain how this technology can improve its accuracy and safety.
2. My personal experience with intraoperative OCT
How long have you been working with the Proveo 8 and EnFocus intraoperative OCT? And how did you come to using the EnFocus intraoperative OCT for your cataract surgeries?
I have been using the Proveo 8 microscope for two years and the EnFocus intraoperative OCT for one year. My surgical activities are dominated by cataract and retinal surgery. Beyond the specific utility of intraoperative OCT in retinal surgery, for which I initially acquired this tool, I rapidly realized that it had considerable potential to improve and upgrade the quality of my cataract surgeries. In my experience, combining the Proveo 8 microscope and EnFocus intraoperative OCT allows an extremely fine analysis in real time and reduces several intraoperative and post-operative complications.
Can you first tell us about your experience with the Proveo 8 microscope?
Proveo 8 has an exceptional optical performance, enabling the surgeon to see more detail with less light. Thanks to its brilliant illumination, the Proveo 8 microscope generates an excellent and steady red reflex throughout the entire cataract procedure, even if the eye is not in line and even if dilation is not optimal, thereby improving visualization and safety. In addition, thanks to the FusionOptics technology, I have a very sharp and focused image during my surgery.
The lighting system of the Proveo 8 has another advantage: it allows the continual adjustment of brightness, with high contrast, high resolution, and natural colors, without chromatic aberrations. The LED also lasts very long, which means less maintenance costs and less time when the microscope is unavailable for use.
One of the hallmarks of cataract surgery is speed; how much faster can you go with this additional device?
Obtaining the best results for the patient depends on being able to see every detail at every time point. The Proveo 8 provides a detailed image with an enlarged focus area, which improves both the vision and the workflow of the surgeon. As such, refocusing is reduced. The use of the EnFocus intraoperative OCT does not slow down the workflow. On the contrary, using the Proveo 8 microscope with EnFocus makes the workflow smooth and comfortable.
The integration of intraoperative OCT controls in the microscope pedal makes it possible to acquire scans very rapidly, at any time, without the need to interrupt surgery. Scans can be obtained at any point in the operation, by a simple press on the foot pedal, handle, or even the touchscreen.
Intraoperative OCT scans provide useful information complementary to that supplied by the already high-quality microscopy images. This makes it possible to confirm or rule out certain complications immediately, such as the presence of a residual fragment hidden behind the corneal edema of one of the incisions or Descemetic detachment, and to assess their extent, and the architecture of the incisions.
Today, intraoperative OCT is not widely used by ophthalmic surgeons. Why do you think it would be any different for cataract surgery? How can intraoperative OCT improve safety in cataract surgery?
After one year of use and about 1,000 cataract operations, I have been able to identify two cases of residual fragments at the end of surgery with intraoperative OCT. Without this technique, I would almost certainly have missed this diagnosis in these two patients. They would probably have required repeat surgery to remove the residual fragment, with all the risks associated with both the residual fragment and secondary surgery.
The EnFocus intraoperative OCT allows immediate confirmation and provides real-time, intraoperative insight into the reaction of the ocular tissue to surgical maneuvers. This makes it possible to adjust the diagnosis and surgical decisions appropriately.
Integrating intraoperative OCT into my cataract surgical activities has made it possible for me to dispel doubts about possible residual fragments or Descemet’s membrane detachment. With the EnFocus intraoperative OCT, these potentially hidden complications are no longer a problem. Combining the use of the Proveo 8 microscope and intraoperative OCT makes it possible to approach cataract surgery with greater serenity and to have even more confidence in the surgical outcome.
Does the Proveo 8 with intraoperative OCT bring particular benefits for difficult cataract surgeries?
When performing cataract surgery on highly myopic eyes, you need to be able to see through the deep anterior chamber clearly. The FusionOptics technology provides a greater depth of field, and excellent visualization of details without the need for frequent refocusing.
Even for the densest cataracts, the Proveo 8 microscope provides a certain degree of red reflex. And, even for total cataracts with no red reflex, intraoperative OCT can be useful for assessing the depth of the residual wall, to improve safety. Furthermore, in these hard cataracts, there is much more corneal edema in the incisions and reduced visibility of potential residual fragments. Using intraoperative OCT allows to see through the corneal edema and identify them quite easily.
Have you ever tried other intraoperative OCT equipments for cataract surgery? What do you prefer about the EnFocus intraoperative OCT over other similar solutions for cataract surgery?
I have not had the opportunity to try other intraoperative OCT devices. However, it is clear that one of the strengths of the Proveo 8 is its upgradability, making it possible to integrate the EnFocus intraoperative OCT at a later point in time. The Proveo 8 can thus be enhanced, at any time, with the integration of the EnFocus intraoperative OCT. From a financial standpoint, it is not always easy to acquire both the microscope and the intraoperative OCT from the beginning. The upgradability of the Proveo 8 platform addresses this critical problem perfectly.
Another important advantage of the EnFocus Ultra-Deep OCT is that it has an exploration depth of up to 11 mm. This makes it possible to acquire images from the cornea to the posterior surface of the lens, which is not possible with other existing intraoperative OCTs.
What's the main reason for which you would recommend the Proveo 8 and EnFocus intraoperative OCT to your peers?
Without any doubt, for the quality of the image, it makes it possible to see really well!
Do you have any other comments or anything else you would like to say about the Proveo 8 and EnFocus intraoperative OCT?
I really like the "surgeon information panel". This screen, located right above the surgeon's oculars, provides access to the main parameters of the microscope in a quick and easy manner. It gives ready access to key information, at a glance, such as the levels of main illumination, retro illumination, magnification, recording, focusing level, OCT status, and mode settings.
3. Studies describing intraoperative OCT in cataract surgery
There are very few studies describing the use of intraoperative OCT during cataract surgery. In the Discover study [6, 7], which included 837 patients, there were 244 cases operated for the anterior segment, and only nine were operated for phacoemulsification. Overall, the authors reported that image acquisition was possible in 98.0% of cases. Among the 244 patients operated on for an anterior segment, intraoperative OCT impacted surgeons' decision-making during surgery in 43.4% of cases. Das et al. reported a descriptive series of 38 eyes from 38 patients operated on for cataracts with intraoperative real-time imaging using the Rescan 700 [11]. Intraoperative OCT was found to be beneficial during all the critical steps of cataract surgery. Authors were able to qualitatively assess wound morphology in clear corneal incisions, in terms of subclinical Descemet's detachments, tears in the inner or outer wound lips, wound gaping at the end of surgery, and in identifying the adequacy of stromal hydration. Deciding the adequate depth of trenching was made simpler with direct visualization. The intraocular lens's final position in the capsular bag and the lack of bio adhesivity of hydrophobic acrylic lenses were also observed [11].
4. Overview of cases performed with intraoperative OCT
4.1 Residual lens fragments assessment with the Proveo 8 EnFocus intraoperative OCT
The residual fragments, when they exist, are often hidden behind the principal and secondary incisions. They are often displaced at this level by the flow of fluid out of the eye. The problem is that corneal edema at the level of the incisions may reduce their visibility. That is why using intraoperative OCT can be greatly beneficial. This technology can see through the corneal edema and easily detect their presence. This can avoid readmission for secondary surgery a few days and weeks later. It reduces all the postoperative complications linked to postoperative residual fragments such as inflammation, Irvin Gass Syndrome, and hypertonia.
What I usually do is perform a 360° circular scan of the anterior segment. Using the microscope pedal, it is possible to go back over the sections to analyze the images.
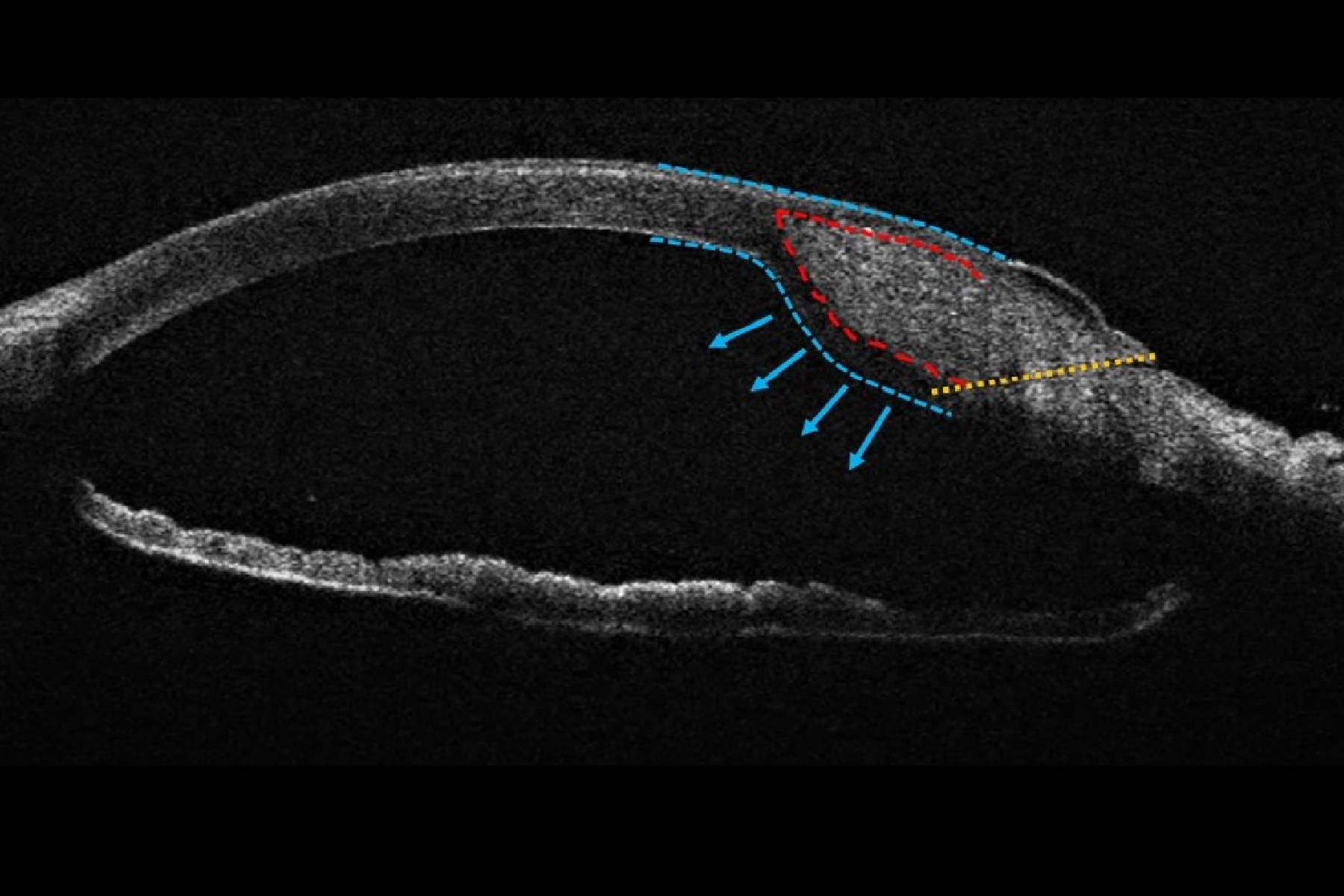
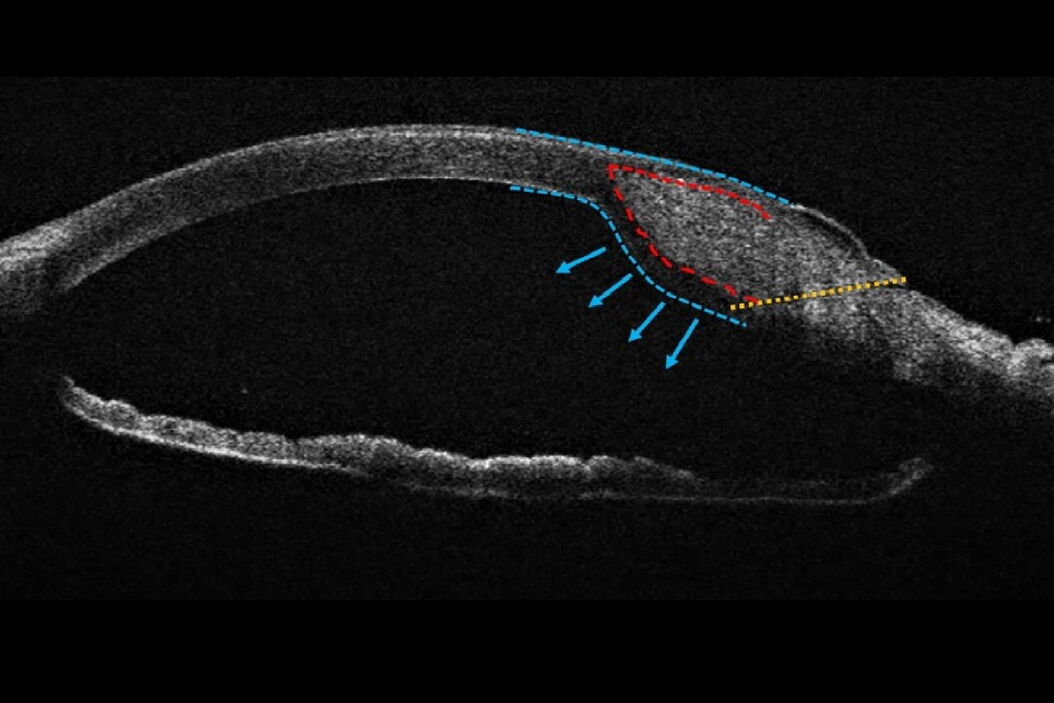
As shown in Figure 1, at the end of the surgery, I had a doubt about the presence of a residual fragment. Thanks to intraoperative OCT, I was able to highlight a residual fragment hidden behind the main incision. It was quite a big fragment hidden behind the edema of the main incision. In the case shown in Figure 2, a small residual fragment was hidden behind the secondary incision.


4.2 Cataract incision analysis using the EnFocus intraoperative OCT
Intraoperative OCT can give accurate and precise information about the incision architecture. We can clearly determine the incision length and the thickness of both superficial and deep flaps. We can perform an analysis both in the longitudinal and transversal sections (Figure 3).
In the case shown in Figures 4 A and B, we analyzed the architecture of the main incision at the end of the surgery, the incision was not very remodeled. In the case shown in Figures 4 C and D, the incision is more remodeled, we could observe a more marked ovalization in the transversal section. In the longitudinal section, we observed a more direct incision with an internal and an external gap.


We can use intraoperative OCT to analyze changes in the incision architecture during hydrosuture. In the case of a sealed incision, we see that the path of the incision disappears, embedded in the corneal edema. The cornea’s anterior curvature remains regular, while a bulging accompanies the corneal edema of the posterior cornea (Figure 5).

When suturing a non-sealed incision, the incision’s path becomes invisible. It is especially noteworthy that the curvature of the anterior face remains almost unchanged. Then, the modification of curvature mainly impacts the posterior face, which becomes a double bump (Figure 6).

4.3 Total cataract case
In total cataracts, there is no red reflex. This makes the sculpting step quite risky because the red reflex becomes visible only when the residual wall thickness becomes relatively thin. This can expose to a risk of early capsular rupture with posterior dislocation of the quasi-total nucleus. Intraoperative OCT can be useful for assessing the depth of the residual wall. This improves safety in these difficult cases.
 and the residual wall is clearly visible (red arrow).")
5. Conclusions
Ophthalmic surgery requires high levels of accuracy and precision for optimal surgical maneuvers and tissue manipulation. Surgical microscopes play an essential role in helping ophthalmic surgeons achieve high precision and improve eye surgery outcomes. In my view, the Leica EnFocus intraoperative OCT imaging system built into the Proveo 8 ophthalmic microscope is cutting-edge technology that provides greater insight during cataract surgery and allows to visualize subtle details, offering real-time intraoperative confirmation of the way tissue reacts during specific surgical maneuvers.
From my personal experience, intraoperative OCT has many advantages and practical applications:
- It allows accurate assessment of the incision architecture throughout the surgical procedure.
- It improves patient outcomes by detecting some intraoperative complications such as residual lens fragments and Descemetic detachment, allowing to resolve the problem immediately and avoid readmission for secondary surgery.
- It also improves safety in hard cataracts by better assessing the depth of the residual wall during sculpting.
Disclaimer: Please note that off-label uses of products may be discussed. Consult with regulatory affairs for cleared indications for use in your region. The statements of the healthcare professionals included in this presentation reflect only their opinion and personal experience. They do not necessarily reflect the opinion of any institution with whom they are affiliated or Leica Microsystems.
About Dr. Tahiri

Dr. Rachid Tahiri, a graduate of Paris VII University, France, is an ophthalmic surgeon working mostly in cataract surgery, retinal surgery, and clinical research. He is a Fellow of the European Board of Ophthalmology (FEBO) and holds a license from the Medical Council of Canada. He has contributed to several articles published in international peer-reviewed journals and has presented numerous scientific studies and posters at international ophthalmology meetings in Europe and the United States. Dr. Rachid TAHIRI is one of the co-organizers of Practical Ophthalmology Webinars, and one of the four artificial intelligence beta testers in France in diabetic retinopathy.



