Introduction
Optical coherence tomography (OCT) is a noninvasive imaging modality based on low-coherence interferometry that provides an in vivo cross-sectional view of the retina. A few years ago, the use of OCT was limited to the preoperative diagnosis as well as to the postoperative follow-up of various diseases [1,2].
More recently, it was brought to the OR as an intraoperative visualization aid to provide further information to the surgeon while operating. Intraoperative optical coherence tomography is an emerging imaging modality. This technique involves the use of OCT during surgery, in order to provide the surgeon with real-time tomographic images.
How did OCT find its way into the operating room?
In 2009, Toth and colleagues at Duke University were the first to perform intraoperative imaging during eye surgery using a new handheld spectral-domain OCT (SD-OCT) system for patients in supine position [2]. The main surgical indications included macular disease, such as full thickness macular hole, epiretinal membrane, and vitreomacular traction. Since standard table-top OCT systems require an upright positioning of the patient and their cooperation, the use of such systems in patients placed in supine positions in the operating room was very limited. Back then, the most common systems used as intraoperative OCT were portable OCT probes that were either mounted to a microscope or used in a handheld fashion. Moreover, prototypes integrated into the microscope were also utilized to allow for true 'real-time' imaging of instrumenttissue interactions. In recent years, advances in intraoperative OCT technology have led to mounted systems that are fully integrated into the surgical microscope.
What are the applications for intraoperative OCT?
Intraoperative OCT has demonstrated to be useful in anterior segment surgery, including corneal transplants and intraocular lens implantation, as well as in vitreoretinal surgery, including epiretinal membrane peeling, perfluorocarbon liquid removal, and subretinal injections [1-4]. Intraoperative OCT was used for conditions such as macular holes, epiretinal membranes, retinal detachments, and retinopathy of prematurity.
Important studies on intraoperative OCT
Two of the most important studies regarding the use of intraoperative OCT focused on revealing whether its use alters the decision-making process during surgical manipulations.
The DISCOVER Study was the first prospective study to report on new OCT systems integrated into ophthalmic surgical microscopes.
In addition, the PIONEER Study was the first large prospective study to report on the use of a portable intraoperative OCT for anterior (275 cases) and posterior segment (256 cases) surgery. Although the study included various surgery indications, the main indication was membrane peeling, in 9% of the cases the intraoperative OCT images provided a peel confirmation, directly contradicting the surgeons' clinical impression [4].
There is still a need to better define the specific applications in which OCT provides the most impact in terms of surgical decisionmaking.
Today’s intraoperative OCT solutions
Currently, there are three systems approved by the US Food and Drug Administration (FDA). The Zeiss Rescan 700 was the first FDA-approved microscope-integrated intraoperative OCT system and is built on the Lumera 700 (Zeiss) microscope platform. Rescan allows visualization of intraoperative OCT data, providing immediate feedback to surgeons through the microscope oculars, without having to look away from the surgical field into an external monitor. This OCT system is also integrated into the microscope foot-pedal, which allows surgeons to control the OCT scan pattern, size, and orientation. The Zeiss Rescan 700 includes Z-tracking and a focus control for image stabilization and quality control.
The Haag-Streit is another intraoperative OCT system (Haag-Streit, Koeniz, Switzerland), which is integrated through the microscope's side port [18]. This system uses the OPMedT (OPMedT, Lubeck, Germany) OCT system and includes a microscope-mounted screen for viewing the OCT images, as well as an external screen for heads-up display. The third system is the EnFocus OCT from Leica Microsystems available with the Leica ophthalmic microscopes like Proveo 8. EnFocus has an increased range of scans that allows for enhanced visualization of pathology [19].
My personal experience with different intraoperative OCT imaging modalities
As a vitreoretinal surgeon, I perform a great variety of vitreoretinal procedures, with the majority of them involving complex subretinal cases and high myopia. I also perform cataract surgery, as well as combined cataract surgery and vitrectomy. Sometimes, I also perform cornea transplant surgery, mainly when it’s related to trauma, as well as valve implantation in secondary glaucoma. Moreover, I have been using intraoperative OCT since 2016 and had the chance to use both imaging modalities from Zeiss and Leica Microsystems. During my personal four-year learning curve with the different intraoperative OCT modalities, I realized that despite the equipment cost and training efforts required to become accustomed to the systems and their imaging software, the added value provided by this technology for ophthalmic surgery and patient outcomes compensates these efforts.
Overview of cases performed with intraoperative OCT
1. Peeling maneuvers
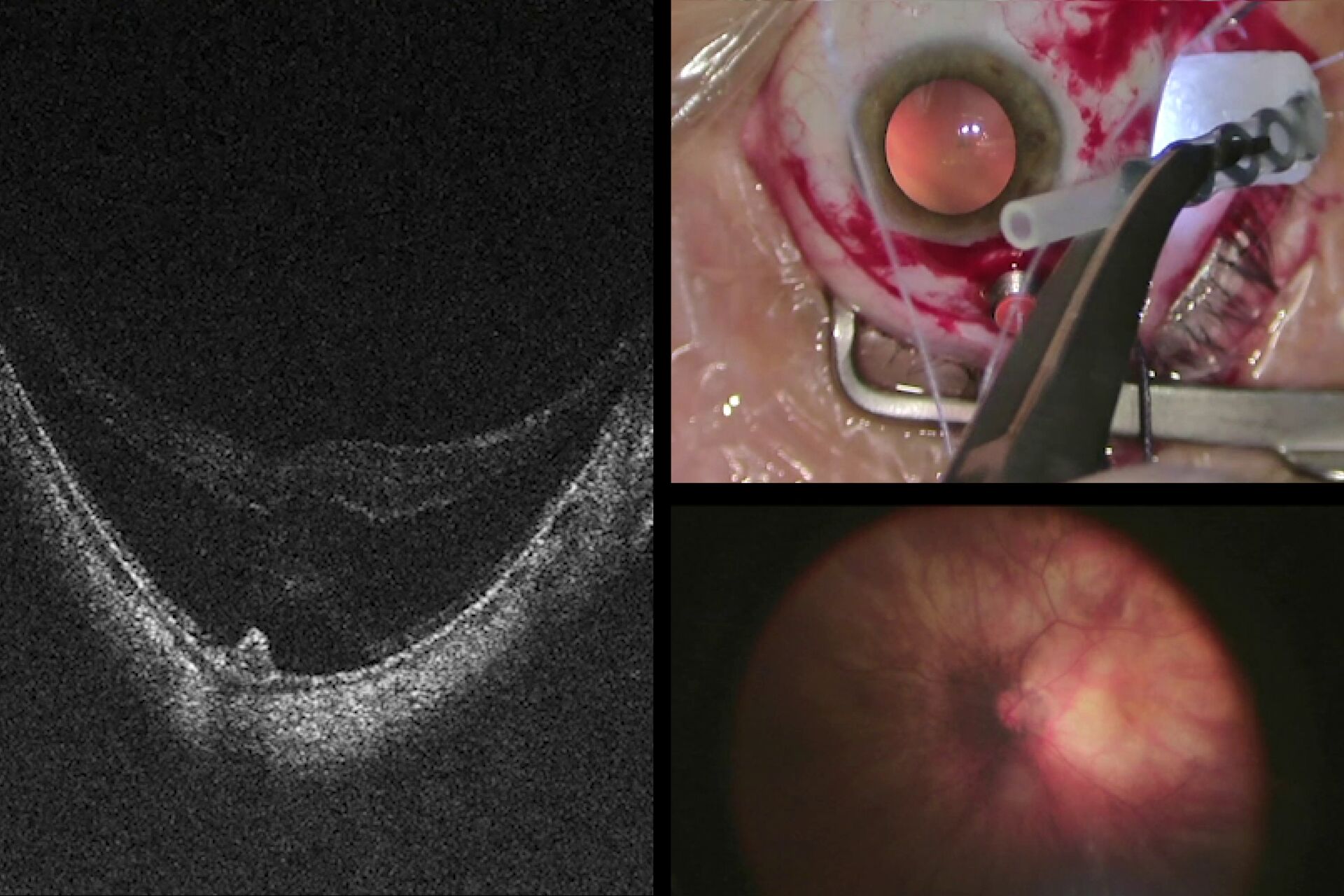
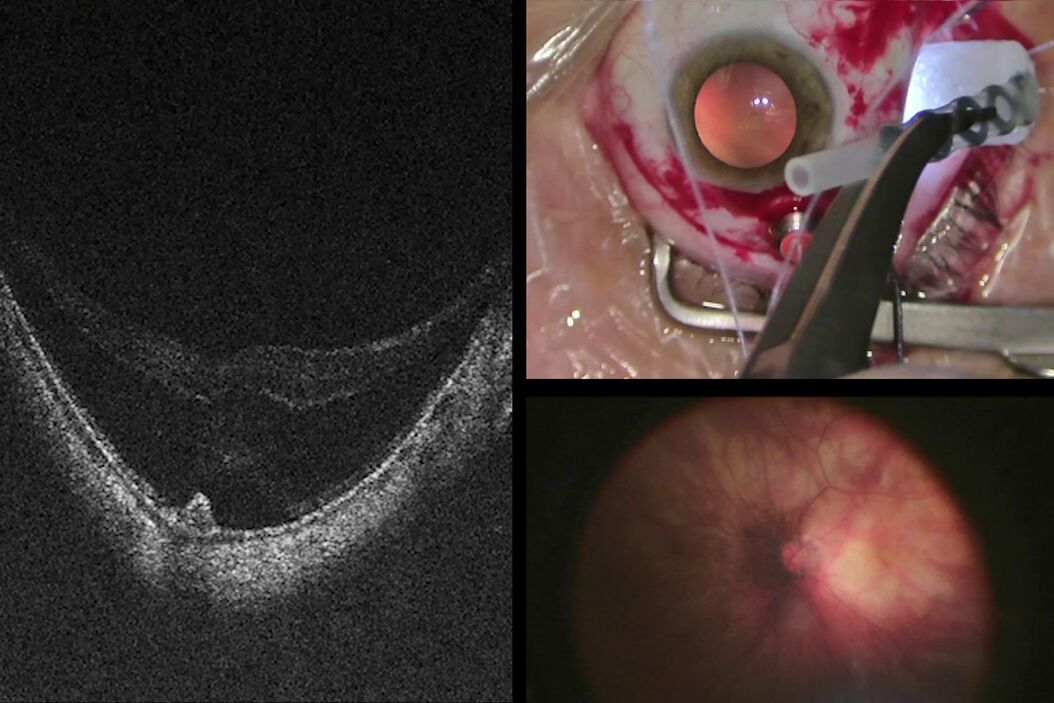
Advantages of intraoperative OCT in operating full thickness macular holes (FTMH) have been reported and published by many authors. Specifically, the main reported advantage is the completeness of peeling, while avoiding membrane residues. While the completeness of peeling can be checked with OCT (Fig. 1) and by using other means, such as staining with dyes, I find OCT to be useful in FTMH cases (Fig. 2) to check whether the internal limiting membrane (ILM) fap is in place under air (Fig. 3). In fact, it has been reported that performing an ILM fap increases the chance of obtaining hole closure [6,7]. This is particularly true in highly myopic eyes. When surgery arrives to the step of fluid-air exchange, the visibility through the microscope is extremely limited. During this step, OCT offers good visibility of details under air and allows the surgeon to determine whether surgery can be stopped or not. allows to determine whether surgery can be stopped or not.


During surgery, the view from the microscope can be limited by intraretinal hemorrhages, edema, and light reflexes. However, intraoperative OCT view is minimally affected by these conditions and, therefore, allows to clearly see the location of the hole in highly myopic eyes, where it is common to observe areas of atrophy at the posterior pole. In case of macular holes, the peeling of membranes is more difficult, because there is no color contrast between the retina and the choroid. It is, therefore, difficult, to judge when to stop peeling, especially since the edges of the hole are hard to see.
Also, the inner limiting membrane (ILM) flap prep and positioning are more difficult. The intraoperative OCT allows confirmation of each maneuver (Fig. 3). Moreover, peeling may provoke bleeding due to pulling of tissue, which can make it difficult to determine whether there is also a retinal break, but OCT can help surgeons to reveal it (Fig. 4).


2. Retinal detachment:
The PIONEER study on intraoperative OCT investigated the amount of subretinal fluid present in retinal detachment cases when perfluorocarbon liquid (PFCL) was injected. The 15 cases included in the study were collected between November 2011 and December 2013. The measurements were then correlated with the anatomical and functional outcomes. In my opinion, the quantification of subretinal fluid under PFCL is only partially meaningful (Fig. 5), since the amount of fluid present under the macula changes once PFCL is exchanged with air. Intraoperative OCT can even be used under air and allows to confirm the presence of subretinal fluid present at the end of surgery, regardless of the type of exchange which has been performed. According to previous published findings, peeling the ILM during macula-off retinal detachment surgeries may help to reduce the risk of a secondary epiretinal membrane formation. In such cases, when I checked the intraoperative OCT images and detected an extremely thin detached fovea during the retinal detachment procedure, I often changed my surgical plan and decided not to perform the ILM peeling (Fig. 6) in order to avoid the risk of inducing an iatrogenic FTMH.


3. Retinal detachment associated with retinoschisis
In 2019, I operated three cases of a retinal detachment associated with a mild vitreous hemorrhage, prior to vitrectomy. In all cases, retinoschisis could be hypothetically assumed. During surgery, intraoperative OCT was enormously helpful in differentiating areas of schisis (Fig. 7) from areas of detachment. In another case of a relapsed retinal detachment secondary to retinoschisis (Fig. 8), which had been previously operated with vitrectomy, PFCL and silicone oil, OCT imaging made it possible to discriminate the differential diagnosis between a retinal break and an intraretinal cyst (Figs. 9, 10), as well as areas of schisis versus subretinal PFCL (Fig. 11). In the same eye, it was very difficult to determine whether the retina was attached under PFCL or whether the case required more retinotomies. Intraoperative OCT imaging helped me determine when and exactly where the retina was (Fig. 12).



.")


PFCL.




4. Macular buckle for retinal detachment in high myopia
Myopic traction maculopathy may present in the form of maculoschisis or macular detachment with or without full thickness or lamellar macular holes (Fig. 13). A macular buckle is one treatment option offered alone or in combination with vitrectomy. To achieve success of the macular buckle procedure, we should aim for a perfect centration in the area of interest. Using the microscope’s panoramic viewing system and fiber optics, we can see the position of the buckle. However, only intraoperative OCT visualization provides a detailed confirmation of the buckle position with respect to areas of interest, such as holes (Figs. 14, 15). Furthermore, only OCT allows accurate visualization of the height of the indentation. This is particularly important under air, when visibility through the microscope is further diminished (Fig. 16). In a few cases, it has been possible to insert a macular buckle without the use of fiber optics, using intraoperative OCT as guidance for the buckle positioning procedure.



.")
5. Submacular surgery and autologous transplantation of RPE and choroid
Various types of exudative and atrophic maculopathies nonresponsive to other treatments can be surgically managed with transplantation of choroid and retinal pigment epithelium (Fig. 17). The long-term results of these types of surgeries have been published [10]. The main steps of surgery are summarized as follows: complete vitrectomy, ILM peeling to prevent macular proliferative vitreoretinopathy (PVR), retinal detachment of the temporal retina, peripheral retinotomy, unfolding the temporal retina on the nasal side, choroidal neovascular membrane (CNV) removal, harvesting of a full-thickness patch of choroid and transplantation of the patch into the macular area, retinal reattachment on the patch with PFCL, and PFCL exchange with either silicone oil or air-gas.
The success of this surgery is linked to the maintenance of the macular area void of macular holes and subretinal residual PFCL. Intraoperative OCT imaging is extremely valuable in determining, when necessary, whether a FTMH was iatrogenically induced during retinal detachment or during ILM peeling. Furthermore, at the end of the surgery, it is very important to detect any undesirable subretinal PFCL bubbles. Also, the correct position and display of the patch in the subfoveal area need to be confirmed directly (Fig. 18). Finally, the OCT also confirms whether the retina is reattached after PFCL-silicone oil exchange (Fig. 19). I had a case where a small PFCL bubble under the retina was detectable only with OCT. The view was not clear due to the condition of the cornea and some opacities in the media, which were not easy to remove.



6. Recurrence of retinal detachment and PVR
In recurrent cases of retinal detachment and, most of all, in cases of proliferative vitreoretinopathy, the retina is more rigid and, in some cases, it is not easy to determine whether it is time to perform a peripheral retinotomy or whether our peeling maneuvers were good enough to release traction. The following questions are usually raised during injection of PFCL: “Is the retina attached or should we peel more? Should we cut the retina?“
Since it is not always perfect, the microscope view alone is not always sufficient to answer these questions. Intraoperative OCT visualization in real-time can be an adjunctive tool to gain valuable information that can influence our surgical plan. For example, in one of my PVR, I could not really see whether the retina was completely attached, due to the edematous aspect that the retina may suffer after PVR peeling. In this case, I needed to decide whether it was necessary to perform a retinotomy, and I used the intraoperative OCT to make the right decision.
7. Vitreous opacities without preoperative OCT
When we operate vitreous hemorrhages or dense vitreous opacities, we commonly do not have the possibility to check the fovea status preoperatively for the shadowing effect that tabletop OCT cannot detect. Therefore, OCT can only be applied intraoperatively, after removing the opacities in the vitreous body. A detailed fovea status check using intraoperative OCT can be helpful in guiding decisions that would be difficult to make otherwise.
The impact of intraoperative OCT use on teaching and education, return on investment and workflow benefits
Teaching and education
In my OR, I always have fellows and observers with me (Fig. 20). I believe that I have managed to offer a better learning experience due to the high-quality images that I work with. In addition to integrated screens on the microscopes, I work with external monitors to share the view of the procedure with my team and students. This also applies to intraoperative OCT images, and I teach fellows how to examine them in order to confirm surgical maneuvers using additional subsurface tissue level information. Overall, understanding the response of live tissue to our maneuvers increases our precision and expertise.

Return on investment
When making the decision of including new technologies into our practice, the cost for an extra instrument must be taken into account by comparing its cost and benefits. In recent years, intraoperative OCT solutions have become more mature, combining state-of-art OCT imaging technology with workflow benefits for the surgeons. If the surgical outcome can be substantially improved with the use of intraoperative OCT, it will likely limit the need for reoperation of the same patient, as well as unnecessary surgical maneuvers. As such, the benefits of using such an instrument easily outweigh its cost.
Workflow Benefits
In the past, workflow in the OR tended to slow down when an OCT image was acquired, since the less advanced portable devices only allow capturing still images. Therefore, when such devices are used during surgery, it is necessary to interrupt the procedure to capture a still OCT image.
However, this problem can be considered as a dynamic variable. It varies over time, as it is directly related to the learning curve of the surgeon and the improvements of the OCT imaging technologies available on the market.
However, OCT imaging with real-time display is extremely important. A surgeon is well aware of how the surgical view can constantly change based on eye positioning, the way the surgical instruments are held, or the way fluids are displaced. Accordingly, moving away from old portable handheld devices to fully integrated, real-time intraoperative OCT imaging solutions brings a whole new approach and improves the surgical workflow tremendously.
The next-generation EnFocus intraoperative OCT built into the Proveo 8 ophthalmic microscope from Leica Microsystems was developed to maximize the surgeons' freedom in the OR. Surgeons can easily supplement their microscope view with bright and sharp intraoperative OCT images at any point during surgery – simply with a tap on the handle, footswitch or touchscreen (Figs. 21, 22). With this imaging system, there is no longer a need for a separate imaging technician. EnFocus OCT provides greater insight during eye surgeries and provides real-time, intraoperative confirmation of the way tissue reacts to surgical manoeuvres.


Another new feature of the EnFocus OCT allows surgeons to automatically find the tissue with the highest reflectivity in the field of view of the microscope. For example, during anterior segment surgery, EnFocus will automatically focus on the cornea. When the microscope is focused further down, the iris will be detected. If there are silicone oil emulsifications in the anterior chamber, which reflects more light than the cornea, the focal plane will be there instead. If a panoramic viewing system is used, the new EnFocus OCT will locate the retina. If the retina is detached or if there is a CNV, EnFocus will set the focal plane at the level of the RPE.
The foot pedal of the Proveo 8 ophthalmic microscope from Leica Microsystems can be fully programmed to allow the surgeon to independently change any parameter of the EnFocus intraoperative OCT. In addition, the surgeon can scan the area of interest in the x and y axes, activate the auto imaging optimization functions, and control focus and contrast of the OCT with the intuitive user interface. Using EnFocus, surgeons can also easily capture videos or still images. Further scan patterns, orientation and size can also be easily be adjusted via the footswitch control.
Conclusions
In ophthalmic surgery, it is essential to receive visual confirmation of the steps taken during each procedure. The microscope view is not always enough to guide our decisions, as it can be impaired due to low contrast CNV, bleeding, and atrophies. Unwanted opacities in the anterior chamber and inability to achieve magnification while maintaining the same image quality is not always possible. Therefore, combining the en face color view of the microscope with the real-time OCT B-scan view, which can be screened slice-by-slice, offers an incredible amount of information regarding subsurface tissue details (Fig. 23).
; en face view (2); OCT b-scan view (3).")
When my team and I observed procedures using the first diagnostic OCT, we did not find this technology useful, as we felt that the slit lamp provided sufficient visualization. Now, we would like to have one OCT system beside every slit lamp. Moreover, when we observed the first angio-OCT, we felt we did not need this system, and believed it could not substitute fluorescein angiography (FA). Now, in many cases, OCT offers extra information in addition to FA.
I believe that intraoperative OCT is likely to follow the same pathway. It has become increasingly useful, as it provides confirmation of the procedure on a subsurface tissue level. And what’s more, intraoperative OCT allows us to see what we cannot see with the microscope alone. As such, we can reliably observe real-time tissue changes and react instantly by adjusting our surgical plan if needed. In my opinion, receiving visual confirmation at every step during surgery is a significant advantage, as it helps enormously in surgical decision-making and diagnosis. In my experience, intraoperative OCT makes the difference between compromise and perfection.



